Do You Go Into Labor Later With Posterior Babies
Posterior
 What is a posterior fetal presentation? The infant's back is spine-to-spine with the mother.
What is a posterior fetal presentation? The infant's back is spine-to-spine with the mother.
Why would posterior position thing in labor? The caput is angled so that information technology measures larger. The height of the caput molds less than the crown.
Baby's spine is extended, non curled, so the crown of the caput is not leading the mode. Baby can't assist equally much during the nascence process to the aforementioned degree as the curled upward baby.
Some posteriors are piece of cake, while others are long and painful, and there are several means to tell how your labor will be beforehand. Afterward this, you may desire to visit What to exercise when….in Labor.
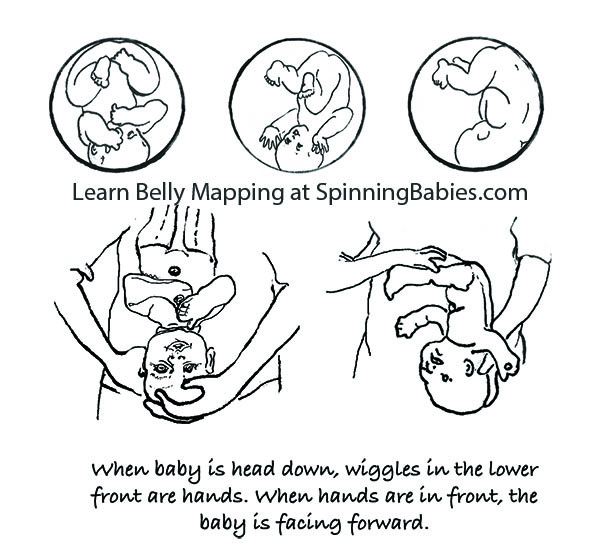
Belly Mapping® Method tips: The Right side of the abdomen is nigh always firmer, but the direct OP baby may not favor one side or the other. Baby'due south limbs are felt in front, on both sides of the eye line. A knee may slide past nether the navel.

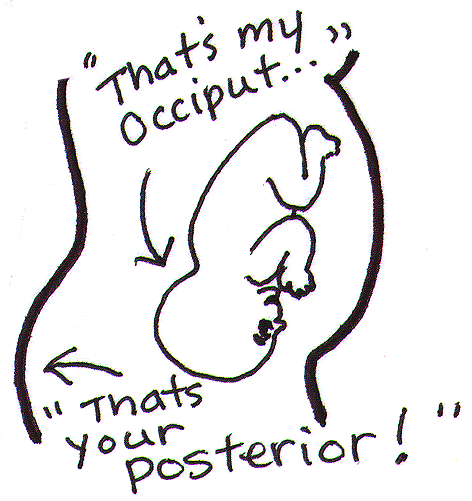
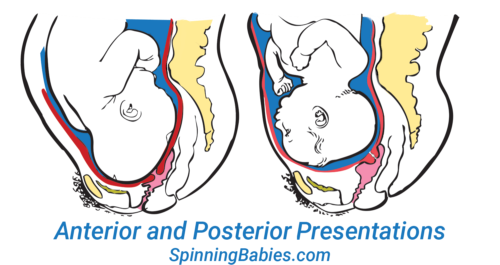
The OP position (occiput posterior fetal position) is when the back of the baby's head is against the mother'due south dorsum. Here are drawings of an anterior and posterior presentation.
Baby Positions
- Overview
- Inductive
- Posterior
- Breech
- Overview
- When is Breech an Issue?
- Belly Mapping® Breech
- Flip a Breech
- When Babe Flips Head Downwardly
- Breech & Bicornuate Uterus
- Breech for Providers
- Belly Mapping®️ Method
- Caput Downward is Not Enough
- Sideways/Transverse
- Asynclitism
- Other Fetal Positions
- Overview
- Oblique Lie
- Left Occiput Transverse
- Correct Occiput Anterior
- Right Occiput Posterior
- Correct Occiput Transverse
- Face Presentation
- Left Occiput Anterior
- OP Truths & Myths
- Anterior Placenta
- Twins
- Body Balancing
- After Baby Turns Caput Down

Look at the above drawing. The posterior baby'southward back is oft extended straight or arched along the mother'due south spine. Having the infant'due south back extended often pushes the babe's chin upwardly.
Attending: Having the chin up is what makes the posterior baby'southward head seem larger than the same baby when it'due south in the anterior position.
Considering the tiptop of the head enters (or tries to enter) the pelvis kickoff, infant seems much bigger by the mother's measurements. A posterior head circumference measures larger than the inductive head circumference.
A large infant is not the same upshot, all the same. The claiming with a posterior labor is that the tiptop of the caput, non the crown of the head leads the fashion.
A baby with their spine straight has less ability to wiggle and so the person giving nascency has to do the work of ii. This can be long and challenging or fast and furious. Also, at that place are a few posterior labors that are not perceived different than a labor with a baby curled on the left.
Why? Anatomy makes the divergence. Learn to work with nativity anatomy to reduce the challenge of posterior labor by preparing with our Three Sisters of ResidueSM and more than.
What to do?
- Three BalancesSM
- Dip the Hip
- Psoas Release
- Virtually everything on this website except Breech Tilt
In Labor, do the above and add,
- Abdominal Lift and Tuck
- Other positions to Open the Brim
- Lunge
- Open the Outlet during pushing
There are iv posterior positions
The direct OP is the classic posterior position with the baby facing straight frontward.Right Occiput Transverse(ROT) is a common starting position in which the baby has a bit more likelihood of rotating to the posterior during labor than to the anterior.Right Occiput Posteriorcommonly involves a straight back with a lifted chin (in the first-time female parent). Left Occiput Posterior places the baby'south dorsum reverse the maternal liver and may allow the baby flex (curl) his or her back and therefore tuck the chin for a better birth. These are generalities, of course. See a fleck more about posterior positions inBelly Mapping® on this website. Want to map your infant'south position? Larn how with theAbdomen Mapping® Workbook.
Pregnancy may or may non prove symptoms. Merely because a adult female'due south back doesn't hurt in pregnancy doesn't hateful the baby is not posterior. Simply considering a woman is quite comfortable in pregnancy doesn't mean the baby is not posterior. A woman can't always experience the baby'due south limbs moving in front to tell if the baby is facing the front.
The 4 posterior fetal positions
Iv starting positions frequently atomic number 82 to (or remain as) directOPin active labor.Right Occiput Transverse(ROT),Correct Occiput Posterior(ROP), and Left Occiput Posterior (LOP) bring together direct OP in calculation labor time. The LOP baby has less distance to travel to get into an LOT position.
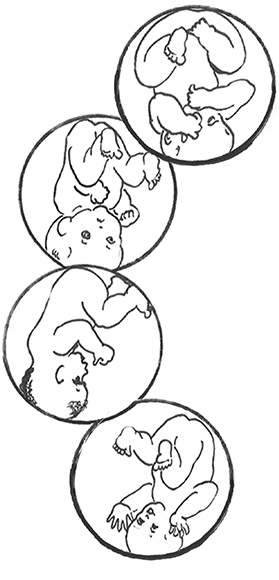
As labor begins, the high-riding, unengaged Right Occiput Transverse baby slowly rotates toROA, working by the sacral promontory at the base of the spine before swinging around to LOT to engage in the pelvis. Most babies go on to OA at the pelvic floor or further down on the perineal flooring.
If a baby engages as a ROT, they may get to OP or ROA by the fourth dimension they descend to the midpelvis. The OP infant may stay OP. For some, in one case the head is lower than the basic and the caput is visible at the perineum, the baby rotates and helpers may come across the baby's head plow then! These babies finish in the ROA or OA positions.
Feeling both hands in front, in ii separate but low places on the abdomen, indicates a posterior fetal position. This baby is Left Occiput Posterior.
Studies estimate fifteen-thirty% of babies are OP in labor. Jean Sutton inOptimal Fetal Positioningstates that l% of babies trend toward posterior in early labor upon admission to the infirmary. Strong latent labor swings almost a third of these to LOT earlier dilation begins (in "pre-labor" or "fake labor").
Recent enquiry shows about 50% of babies are in a posterior position when agile labor begins, but of these, iii/4 of them rotate to anterior (or facing a hip in an occiput transverse, head down position.
Jean Sutton's observations, reported in her 1996 volume, indicates that some babies starting in a posterior position volition rotate before arriving to the hospital. Ellice Lieberman observed well-nigh posteriors will rotate out of posterior into either anterior or to facing a hip throughout labor. Merely 5-eight% of all babies sally directly OP (13% with an epidural in Lieberman'south study). At least 12% of allcesareansare for OP babies that are stuck due to the larger bore of the OP head in comparing to the OA head. It's more mutual for ROT, ROP, and OP babies to rotate during labor and to sally facing back (OA). Some babies become stuck halfway through a long-arc rotation and some volition demand a cesarean anyway.
The 3 inductive starting positions for labor
 The three anteriors —LOT, LOA, and OA — are all platonic fetal positions for the kickoff of labor. Both LOA and OA require less rotation than LOT and may lead to a faster labor, only they may also be less mutual. Generally, very few midwives or doctors will pay strict attention to the actual caput position, leading to the LOT baby often beingness referred to equally LOA or only OA.
The three anteriors —LOT, LOA, and OA — are all platonic fetal positions for the kickoff of labor. Both LOA and OA require less rotation than LOT and may lead to a faster labor, only they may also be less mutual. Generally, very few midwives or doctors will pay strict attention to the actual caput position, leading to the LOT baby often beingness referred to equally LOA or only OA.
Why not ROA? ROA babies may have their chins upwards and this deflexed position may lengthen the course of labor. Less than 4% of starting positions are ROA, co-ordinate to a Birmingham study. This might not be ideal for first babies, but is not a posterior position either.
The spectrum of ease across posterior labors

There is a spectrum of ease across posterior labors. It's not a bell curve, though; like shooting fish in a barrel posteriors are non equally common every bit challenging ones. Usually, babies turn after many strong contractions. Without help, almost one-half of women volition requite birth to their posterior babies. The techniques chosenThe Fantastic Fourare probable to improve mothers' and babies' ease of nativity! Larn these techniques that volition assist you avoid unnecessary surgery for your baby's birth by watching theSpinning Babies® Parent Course video:
Parent Class
Babe'southward posterior position may thing in labor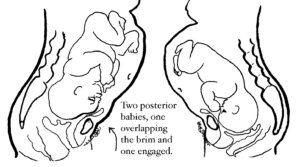
With a posterior presentation, labor may or may non be significantly affected. There is a spectrum of possibilities with a posterior baby. Some women will not know they had a posterior baby considering no 1 mentions it. Either the providers didn't know, or didn't notice. If labor moved along, they may not have looked at fetal position clues since at that place was no reason to effigy out why labor wasn't progressing. If a woman didn't have dorsum labor (more pain in her back than in her abdomen), the provider may not have been "clued into" babe's position.
Some posterior babies are born in less than 8 hours and position did not slow down labor. Some posterior babies are born in less than 24 hours and position did not slow down labor enough to exist out of the norm. Some posterior babies are built-in in less than 36-48 hours without the need for interventions.
Some posterior labors are manageable when women are mobile, supported, and swallow and drink freely, as needed. Some posterior labor needs extra support that a well-trained and experienced doula may provide, but that typically a mate or loved one would not have the skills or stamina to keep upward with. Some posterior labors progress merely with the help of a highly-trained pregnancy bodyworker or deep spiritual, or otherwise a non-conventional model of intendance. Or, they seem simply able to terminate with medical intervention.
Some posterior labors are served by an epidural, meaning the pelvic floor relaxes enough for the infant to rotate and come out. Some epidurals, on the other mitt, make it so that a woman tin can not cease the nascency vaginally.
NOTE: Parents should know — some birth researchers, like Pediatrician John Kennell, are seriously asking whether a mother's epidural turns off her body's release of pain-relieving hormones which a baby relies on during childbirth. Some babies tin't turn and can't be built-in vaginally and must be born pastcesarean. This is a spectrum of possibilities. I've seen every one of the in a higher place possibilities several times and can add the wonderful experience of seeing a adult female laughing pleasurably and squatting while her posterior baby slid out on to her bedroom flooring.
Possible posterior effects, some women volition have one or two and some will have many of these:

The brow that overlaps the pubic bone later labor starts must turn and drop into the pelvis to allow the birth to happen naturally. A cesarean finish of the labor is possible. Wait at Abdominal Lift and Tuck in Techniques to guide you to solutions for easier engagement and progress.
- Longer pregnancy (some research shows this and some doesn't)
- The amniotic sac breaking (water breaks, membranes open, rupture of membranes) before labor (one in 5 OP labors)
- Non starting in time earlier inductionis scheduled
- Labor is longer and stronger and less rhythmic than expected
- Start and stoplabor pattern
- The baby may not engage, even during the pushing stage
- Longer early labor
- Longer agile labor
- Back labor (in some cases)
- Pitocin may be used when labor stalls (but a snoring good residue followed by oatmeal may restore a contraction pattern, too)
- Longer pushing phase
- Peradventure a woman has all three phases of labor lengthened by the OP labor or ane or 2 of the three phases listed
- Sometimes the baby's caput gets stuck turned halfway to anterior – in the transverse diameter. This may be called a transverse arrest (not atransverse lie).
- More likely to tear
- More likely to need a vacuum (ventouse) or forceps
- More likely to demand acesarean
These effects are in comparing to a baby in theleft occiput anteriororleft occiput transversefetal position at the get-go of labor.
Who might have a hard time with a posterior baby?
This family just had a fast posterior birth of their second kid! Ease in labor includes other factors across baby position.
- A starting time-time mom
- A first-fourth dimension mom whosebabe hasn't dropped into the pelvis by 38 weeks gestation(ii weeks before the due date)
- A woman with anandroid pelvis("runs like a boy," ofttimes long and lanky, depression pubis with narrow pubic curvation and/or sitz basic shut together, closer than or equal to the width of a fist)
- A woman whose baby, in the third trimester, doesn't seem to change position at all, over the weeks. He or she kicks in the womb and stretches, just whose torso is stationary for weeks. This female parent'due south broad ligament may be so tight that she may be uncomfortable when infant moves.
- A adult female who has an epidural early in labor (data supports this), before the baby has a adventure to rotate and come down.
- A woman who labors lying in bed
- Low-thyroid, depression-free energy adult female who has gone overdue (this is my observation)
- A woman who lacks support by a at-home and assured adult female who is calming and reassuring to the birthing mother (a doula)
- A woman put on the clock
- A adult female who refuses all aid when the labor exceeds her ability to physically sustain her self (spilling ketones, dehydration, unable to eat or rest in a labor over Ten amount of hours which might exist 24 for some or 48 for others)
- A woman whose nascency team can't match an appropriate technique to the needs of the baby for flexion, rotation, and/or descent from the level of the pelvis where the baby is currently at when stuck
Who is likely to take an easy fourth dimension with a posterior babe?
- A 2d-time mom who's given nativity readily before (and pushing went well)
- A posterior baby with a tucked chin on his or her mama'south left side witha round pelvic skirt
- An average-sized or smaller baby
- Someone whose posterior baby changes from right to left later on doing inversions and otherbalancing work, though the babe is notwithstanding posterior
- A adult female with a baby in the Left Occiput Posterior, peculiarly if the baby's chin is tucked or flexed
- A woman who gets bodywork, myofascial release, etc.
- A woman whose posterior baby engages, and does not have anandroid (triangular) pelvis or a small-scale outlet
- And of all of these, what is necessary is a pelvis large enough to arrange the infant's extra caput size
- A woman who uses active birthing techniques — vertical positions, moves spontaneously and instinctively or with specific techniques from Spinning Babies®, and other good advice
- A woman in a counterbalanced nervous country, not and so alarm and "pumped upward," on guard, etc.
Whatsoever adult female may also take an easier fourth dimension than public opinion might point, too, just because she isn't on this listing. Equally, just because she is on the "difficult" listing doesn't hateful she volition take a hard time for sure. These are general observations. They are neither condemnations nor promises. Overall, some posterior babies will need assistance getting built-in, while some posterior babies are born easily (piece of cake existence a relative term).
Let'south not be ideological almost posterior labors.
While nigh posterior babies do eventually rotate, that can still hateful there is quite a long wait – and a lot of concrete labor during that wait. Sometimes it means the doula, midwife, nurse, or doctor is asking the mother to do a diversity of position changes, techniques, and fifty-fifty medical interventions to help finish the labor. Patience works for many, just for some acesareanis really the simply way to be born. ReadWhat To Do When…in Labor.
What causes a baby to be posterior?
In that location is a ascent incidence of posterior babies at the time of birth. We know at present that epidural anesthesia increases the charge per unit of posterior position at the time of nascence from about 4% (for women who don't choose an epidural in a university nascence setting) up to nearly 13% (Lieberman, 2005). Low thyroid function is associated with fetal malposition such as posterior or breech. (Run acrossInquiry & References.)
Virtually babies who are posterior early in labor will rotate to inductive once labor gets going. Some babies rotate late in labor, fifty-fifty just before emerging. Studies such every bit Lieberman's show that at any given phase of labor, another twenty% of posterior babies will rotate so that but a small number are withal posterior as the head emerges.
My observations are that the majority of babies are posterior before labor. The high numbers of posterior babies at the end of pregnancy and in the early phase of labor is a change from what was seen in studies over ten years former. Peradventure this is from our cultural habits of sitting at desks, sitting in saucepan seats (cars), and leaning back on the burrow (slouching). Soft tissues such equally the psoas muscle pair or the broad ligament also seem to be tight more than often from these postures, from athletics (quick stops, jolts, and falls), from accidents, and from emotional or sexual assail.
Being a nurse or bodyworker who turns to intendance for people in a bed or on a tabular array will also twist the lower uterine segment (along with some of the previously mentioned causes). This makes the babe accept to recoup in a womb that is no longer symmetrical. Less often, the growing babe settles face-forrad over a smaller pelvis, or a triangular-shaped pelvis (android). At the end of pregnancy, the baby's forehead has settled onto a narrower than usual pubic bone, and if tight round ligaments hold the forehead there, the babe may take a tough time rotating. These are the moms and babies that I'm almost concerned with in my piece of work at Spinning Babies®. A baby that wasbreechacross week xxx – 34 of pregnancy volition flip head down in the posterior position. A woman with a history of breech or posterior babies is more than likely to take a breech or posterior baby in the next pregnancy. However, she may not accept an as long labor.
The best way to tell if your baby is OP or not, usually, is if you lot feel little wiggles in the abdomen correct above your pubic bone. These are the fingers. They'd feel like little fingers wiggling, not similar a big thunk or grinding from the head, though you might experience that, also. The lilliputian fingers volition be playing by the mouth. This is the easiest indication of OP. The wiggles volition be centered in the middle of your lower belly, close to the pubic bone. If y'all experience wiggles far to the right, near your hip, and kicks above on the right, just not near the center and none on the left, then those signal anOAorLOTinfant (who will rotate to the OA easily in an active nascency). Later this, you might go toWhat to practice when…in Labor.
Check out our current references in the Inquiry & References section.
Videos
Daily Essentials
Daily Essentials can be good daily throughout pregnancy to assist bring balance and comfort — and an easier, shorter birth.
Spinning Babies® Parent Form
Spinning Babies® Parent Form provides clear instructions on how to use Spinning Babies® for a more comfy and confident pregnancy and labor.
Do You Go Into Labor Later With Posterior Babies
Source: https://www.spinningbabies.com/pregnancy-birth/baby-position/posterior/
0 Response to "Do You Go Into Labor Later With Posterior Babies"
Post a Comment